VAERS (Vaccine Adverse Event Reportin System) is a voluntary reporting system for adverse events from vaccines. It was created in the 1990's in response to the National Childhood Vaccine Injury Act, which shielded vaccine manufacturers from liability in the event of adverse events. It is a voluntary reporting system, so will not capture every adverse event. In fact, it is estimated that less than 1% of adverse events are actually reported to the system. Here is some more discussion on the problem with VAERS reporting. Steve Kirsch estiamted the under reporting factor (URF) as 41, meaning that you can generally take the number of adverse events reported in VAERS by 41 and get the actual number. Here is the detailed discussion of this estimate.
Here is a discussion from James Lyons-Weiler, PhD about the issue of VAERS reporting and the bias for doctors to underreport, or not trust those reports at all. Here is a whistleblower stating that 90% of her hospital admissions were vaccinated even though the community she was in had 50% vaccine coverage, and the FDA and CDC completely ignored this report. Here is another great article on pharmacovigilance on the pandremix vaccine. Here is a similar article on pandremix.
One of the first statements pro-vaxxers say in response to VAERS is that there is no proof of causation and therefore we have no idea if the deaths reported are from the vaccine. This study (with this summary) from Germany shows autopsies done on 10 people who died after covid vaccination. the pathologists found that 7 out of the 10 were confirmed to have died directly from the vaccine. More discussion is found here from the pathologists on the worthlessness of death certificates and how vaccine causes of deaths aren't reported. The report also discusses coorboration of another German pathologist that found that conservatively 30-40% of deaths occuring after vaccination were due to the vaccine itself.
There are some clever methodological tricks that Big Pharma uses to make their vaccines seem either more efficacious or more safe. Here here and here are examples of a TDaP vaccine Randomized Control Trial (RCT), which is the "gold standard" of showing causation. In other words, if you want to show if a vaccine is truly effective and safe in as close to a real life scenario as possible, you would want to do a RCT. The pro-vaccine side will claim that RCT's are done, even though the anti-vax side claims that they haven't been done. The reason for this discrepancy is that while RCT's are done, the placebo that is used, in the case of the above studies, are actually other TDaP vaccines. By comparing one vaccine to another vaccine, you cannot get accurate safety signals to compare an unvaccinated group to a vaccinated group, because both groups are being injected with vaccines with similarly toxic ingredients. Here is a more egregious study that claims to be able to make a claim on safety of the vaccine in pregnant women, when they don't even use a control group at all.
Another trick that they use is the use a "placebo" that actually contains all of the same adjuvants and toxic excipients as the vaccine, having the same effect where safety data cannot be reliably gleaned by comparing the two groups. Quote "The placebo had the same constituents and identical appearance as the active vaccine, but did not contain the vaccine virus." This is what anti-vaxxers mean when they say that and RCT comparing vaccinated to unvaccinated groups has never been done. The Gardasil vaccine trials used an aluminum adjuvant placebo as well.
Here is an article from forbes outlining how the COVID-19 trials were designed to succeed beforehand. In the Pfizer Trial, pg.41:
"Among 3,410 total of suspected but unconfirmed COVID-19 in the overall study
population, 1,594 occurred in the vaccine group vs. 1,816 in the placebo group. Suspected
COVID-19 cases that occurred within 7 days after any vaccination were 409 in the vaccine
group vs. 287 in the placebo group. It is possible that the imbalance in suspected COVID-19
cases occurring in the 7 days postvaccination represents vaccine reactogenicity with symptoms
that overlap with those of COVID-19. Overall though, these data do not raise a concern that
protocol-specified reporting of suspected, but unconfirmed COVID-19 cases could have masked
clinically significant adverse events that would not have otherwise been detected."
Also, in pg 18: 311 vaccine recipients excluded due to protocol deviations, only 60 in placebo group. Statistically unlikely.
Let me explain the significance of these passages. The first passage comes from the discussion at the supplemental materials and describes the number of people in the vaccinated group vs unvaccinated group at 7 days that were presenting with COVID-19 symptoms. These were NOT included in the final anaylsis, presented in table 7 page. 24. This is where they get their 95% relative risk reduction, where 9 in the vaccinated group were confirmed COVID-19 vs 169 confirmed COVID-19 in the placebo group. However, when you include the total number of people that are presenting with COVID-19 symptoms between both groups, you see that in the vaccine group, there are 9 + 409 = 418, vs the placebo group there is 169 + 287 = 456. What you see here is an insignificant difference in symptomatic cases, but Pfizer simply was able to choose to end the study before these remaining "suspected cases" were able to be tested. They were able to "cherry pick" by waiting until they got their 95% reduction at 95% confidence interval, and immediately ended the trial and submitted the data for emergency use authorization. Which of course, was approved by FDA, as it is simply a regulatory captured wing of the pharmaceutical industry. See Conflicts of Interest. The second passage on page 18 is to point out a sense of skepticism on the fact that there was such a large difference in protocol deviations between the vaccinated and placebo group. You can read about some more issues with this trial here
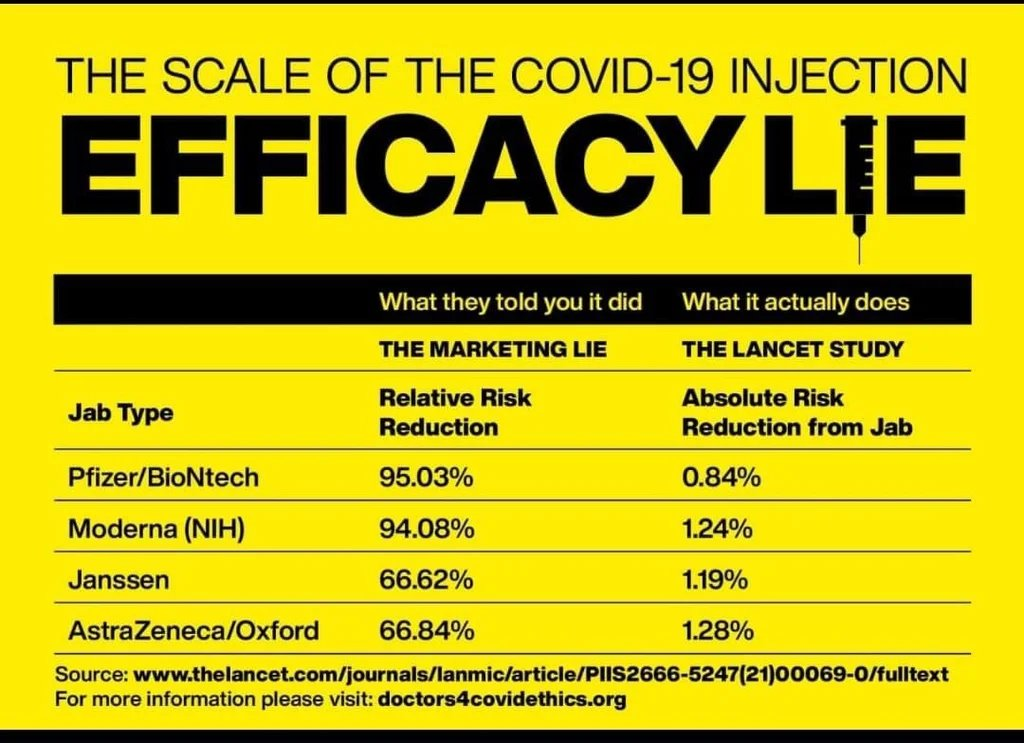
Another quick thing to add on the vaccine trials is the subject of using relative vs absolute risk reduction as a way to make more impressive headlines and marketing ploys. This explains the difference of absolute vs relative risk reduction. Here is the comparison of relative to absolute risk reduction.
In fact, in this video, you can see how a mother speaking on her daughter that was paralyzed during the pfizer vaccine trial, who does not seem to have been included in the data on adverse events. Here is a report on a whistleblower calling into question the veracity of the data from the pfizer trial, unwillingness of FDA to respond to issues and even threats from staff members for reporting certain issues. While were on the topic of misreporting, a cdc whistleblower stated that he was instructed to destroy evidence that there was a link between vaccination and autism.
Here is another cute tactic that the CDC used. They claimed that only 12.6% of the women suffered miscarriages, which is consistent with data from typical pregnancies pre-pandemic. However, the reason they can state this is, again, a methodological tactic in the design of the study. This is because they designate miscarriages as only happening prior to week 20 of a pregnancy. They claim that out of the 827 participants, 104 had miscarriages. However, the population that were vaccinated before their 20th week of pregnancy was only 127 women, so that means in reality, 104/127 women suffered miscarriages, or 82%, NOT 12.6%. This is how to lie with statistics at its finest. Here is another example of gaming statistics for favorable marketing schemes. "Thus, the reported pooled efficacy against CIN 1-3 in Gardasil post-licensure trial gave a highly misleading impression about the true clinical value of the vaccine, given that the vast majority of the lesions within the trial population would have comprised of CIN 1 lesions."
Another tactic to mention is the unblinding of study participants. They (vaccine manufacturers) did this in the most recent trials. Basically, once pfizer and moderna had their data after around 7 days that showed 95% efficacy and got approved for emergency use authorization, those in the placebo group were notified that they had received placebo (unblinding) and were asked if they would like to receive the actual vaccine source. Moderna provided data that "As of April 13, all placebo participants have been offered the Moderna COVID-19 Vaccine and 98% of those have received the vaccine.". So their long term trials no longer have a control group. The mainstream rationale for this is to be "fair" to those that didnt receieve the vaccine, as it would be unethical to keep them from having a potentially life saving prophylactic. This is the same rationale that they use to avoid using RCT with saline placebos.
Yet another tactic used, that is used in many unvaccinated vs vaccinated analyses on the efficacy of the COVID vaccine (see Manufacturing a Pandemic), but in this case was used in the vaccine trials as well was to not count cases of COVID-19 that occured before 7 days (in the case of the primary endpoint) and before 14 days (secondary endpoint). The rationale for which is that adverse events to vaccines and sickness after vaccination is well known to mostly occur immediately after the vaccination, referred to as the negative phase. In the case of data analyses comparing vaccinated to unvaccinated people in real life, they will count any cases before 14 days after vaccination as an "unvaccinated" person, and also at any time after only 1 dose, you are considered unvaccinated, which will greatly inflate the unvaccinated statistic as there will be many adverse events among the vaccinated at this point. Please see Manufacturing a Pandemic
Another trick described here by Public Health Scotland. They present the deaths due to covid as a rolling tally since the vaccine was released in dec 2020. Because of this, the number of unvaccinated are much higher than vaccinated, but thats because in the time of this report, they are counting all the deaths from a time when the vaccine uptake was below 9%. So naturally, most the deaths will be among the unvaccinated. That article contains an analysis that show that 87% of the deaths were among vaccinated people, even given the high vaccination uptake in Scotland. This same sleight of hand was pulled by the CDC Director Rochelle Walensky claiming "over 97% of people who are entering the hospital right now are unvaccinated" source. She admits later that this data was from jan-june, a time when most americans had not been vaccinated.
This article discusses the fact that measles cases after measles vaccines are not counted as measles cases. This is a good article on the "Chrysalis Effect", explaining a way to game studies in your favor. Amazingly, we can see an admission in a paper from 1994 about a MMR vaccine program in Finland and the supposed "eradication" of the disease. "The 99% decrease in incidence of the three diseases was accompanied by an increasing rate of false positive clinical diagnosis". In other words, amazingly, they are stating that they are still seeing measles cases, but that they are now considering them "false positives", so they are no longer counted as measles cases. No wonder they are seeing such a decline!. Also this article by Suzanne Humphries responding to a "debunking" shows measles reclassifications.
To summarize, measles cases were reclassified as vaccine-induced measles that the vaccine would often induce, which artificially decreased the measles case rate. It would seem to prevent symptoms, but some long term studies show that measles is beneficial in the long run to have. The attitude in the 1950s was also to have "measles parties" and that it was a very mild illness. Very very rarely did you have problems arise from measles. The study below also shows that even though it seemed "measles-induced" encephalitis decreased, total encephalitis stayed the same, implying it was a reclassification problem. "The spectrum of encephalitis in children has changed due to vaccination programs. The incidence, however, appears to be about the same due to increasing frequency of other associated old and new microbes." source
This article references the fact that 1 in 40 reported cases of measles went on to actually being laboratory confirmed cases of measles. "Last year, WHO (2) stated that measles mortality in Africa had slashed the death rate from measles by 91% since 2000. This 91% is an artifact figure, because before 2000, measles in Africa was "estimated", while after 2000, notifications were only accepted after being laboratory proven. In 2000, WHO implemented a system of laboratories (3) specifically to diagnose measles, and provide the laboratory confirmed cases which are now the basis of WHO data. Look at pages 2, and 14. On page 14, 14,185 cases were reported in 2006, but after blood testing, 9,764 were "discarded". That's an immediate 69% drop in cases, because they are no longer relying on doctor's eyes. On page 2, of 14,185 cases, 3,257 were accepted, leaving a balance of 10,928 discarded measles cases which equals 77% which were NOT measles after being blood tested, but which would have been accepted on the pre- 2000 measles notification system. Comparing data from laboratory-confirmed blood tests after 2000, with pre-2000 guessing, and then claiming a 91% decline, is not a valid scientific comparison." sourceIn the first 6 years of life your child in the USA receives the following in the vaccine schedule
17,500 mcg 2-phenoxyethanol
5,700 mcg aluminum
Unknown amounts of fetal bovine serum
801.6 mcg formaldehyde
23,250 mcg gelatin
500 mcg human albumin
760 mcg of monosodium L-glutamate
Unknown amounts of MRC-5 cells
Over 10 mcg neomycin
Over 0.075 mcg polymyxin B
Over 560 mcg polysorbate 80
116 mcg potassium chloride
188 mcg potassium phosphate
260 mcg sodium bicarbonate
70 mcg sodium borate
54,100 mcg of sodium chloride
Unknown amounts of sodium citrate
Unknown amounts of sodium hydroxide
2,800 mcg sodium phosphate
Unknown amounts of sodium phosphate monobasic monohydrate
32,000 mcg sorbitol
0.6 mcg streptomycin
Over 40,000 mcg sucrose
35,000 mcg yeast protein
5,000 mcg urea
Other chemical residuals
This is a vast topic and there are many good all in one sources that already exist on the topic. A large portion is going to be dedicated to the COVID vaccine as it has a LOT of studies and information out on it right now for obvious reasons. I will try to talk about some of the general aspects of safety first. As shows above, there are verifiably toxic components in all vaccines, the most notable in recent years being aluminum and mercury. The typical talking point among the pro-vaccine side is that the levels of these toxins are so low they will not cause problems. They typically say that the amount of mercury in fish and other foods is much higher than the amount of mercury in vaccines. The problem with this point of reasoning is two-fold. 1) This obviously does not excuse the very real problem of excess mercury in food and how that can be very toxic, so they can BOTH be problems, but 2) the toxic levels set by the EPA that place the amount of mercury in vaccines in the "acceptable" level are based on ORAL ingestion of mercury, through the gastrointestinal tract. It should be clear to anyone that eating 10mcg of mercury will be tolerated vastly different from a toxicological point of view than injected directly into muscles transdermally (or god forbid intravenously, which does mistakenly happen many times).
Another problem is the misconception that toxic components will not make their way into the brain due to the permeability of the Blood Brain Barrier (BBB). I will now present studies that show that there is reason to believe that many toxins from these vaccines can find themselves into the brain. Here and here we see a study showing low levels of mRNA (a component in the COVID vaccines) could be detected in all examined tissues except the kidney (in rats). This included heart, lung, testis, and also brain tissues, indicating that the mRNA/LNP (lipid nanoparticle) platform crossed the BBB, although to very low levels (2-4% of the plasma level). Here is a discussion of LNP's being able to cross the BBB. Here is a study on Lipid Nanoparticles being used specifically to try to cross the BBB and target the brain. "Lipid based formulations can be designated as the current and future generation of drug delivery systems as these possess tremendous potential to bypass BBB and reach the target site due to their small size and ability to dodge the reticular endothelial system." It's worth noting that the discussion of Lipid Nanoparticles (PEG) is specific to the COVID vaccine. It is used in COVID vaccines because the LNP are supposed to engulf the mRNA molecules, and due to their ability to cross cell membraines allow the mRNA to enter the cells. The problem with including these particles that are so readily able to cross the BBB is that certain toxins and contaminants can make their way into the brain, especially if you have a contaminated batch (see Quality Control). Given these LNP ability to engulf other molecules, including metal contaminants found in vaccines, these metals can make their way into the brain. We will also get into the specific toxicity of PEG later.
This is not the only mechanism for toxins in vaccines to make it into the brain, however. We see here that despite what was believed prior, lympatic vessels were found to exist in the brain. Here and here we see that the components in vaccines are known to remain near the site of injection and immediately travel to the lymph nodes. This study shows that aluminum is phagocytosed (englufed) both in vivo (in organisms) and in vitro (in petri dishes) by macrophages (immune cells). This study shows that macrophages can cross the BBB. Thus, macrophages can engulf these neurotoxic excipients in vaccines and transport them into the brain. This, this, and this are more studies that shows that macrophages engulf aluminum particles, and their ability to transport them to the brain. You can read more of the vast body of evidence linking mercury and aluminum to autism here
When it comes specifically to the covid vaccine, we can look at the studied toxicity of PEG. Here are a few studies on this topic:
The mRNA-LNP platform's lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory
Dangerous immune response from PEG
Animal studies show PEG responsible for anaphylaxis and cardiovascular collapse
PEG induced anaphylactic reaction during bowel preparation
Polyethylene Glycol-Induced Systemic Allergic Reactions
Pre-existing anti-PEG antibodies are associated with severe immediate allergic reactions to pegnivacogin, a PEGylated aptamer
Polyethylene glycol as a cause of anaphylaxis
Anaphylactic Shock Caused by Ingestion of Polyethylene Glycol
There are also many studies about the adverse events from the covid vaccine. See this page for the list of studies on this topic. The page includes a list of adverse events to the vaccines, many studies investigating them, and a collection of stories online of people dying and being injured from the vaccine. This slidehow by Steve Kirsch is very informative and covers the issue of both safety and effectiveness of the COVID vaccines. This page collects a multitude of examples of deaths rising substantially immediately after vaccines are rolled out, and while it is a correlation, the sheer number of examples and exactness of timing is almost too obvious to ignore.
There is more testimonies from people where one can deduce that there may be a serious death toll to this recent vaccine rollout that aren't being reported. This data from funeral site shows sharp rise in excess deaths in recent months. These articles are showing that ER's are filled with patients that don't have "COVID". It doesn't take much to deduce that these patients may in fact be suffering from adverse events from the vaccines.
In Taiwan, the deaths from the covid vaccine exceed deaths from COVID itself. These are examples of various countries that decided to pause or stop the vaccines rollout to various groups. Another
To zoom back out to other vaccines besides the covid vaccine, here are some resources on the safety of various vaccines. This article talks about 6 out of 10 vaccines that are studied actually increases as opposed to decreasing deaths. Here is an article on the smallpox vaccines damage to military members, and another one here. here is an article on how various vaccines can cause damage.
This paper discusses the link between vaccines and sudden infant death syndrome. This one discusses seizure risks from vaccinations. This paper shows that infants that are "undervaccinated" have less doctors office visits than children that have more vaccines. This is a similar study that compares trends of hospitalizations and mortalities among infants based on the amount of vaccines and age of vaccination.
The polio vaccine was a particular disaster. The Cutter Incident was the most famous admitted botched vaccination program that killed and paralyzed many children due to "contaminanted" batches. It is in fact today admitted in the mainstream that there are more polio cases now caused by vaccine than by wild virus. Four Times in History Vaccines Failed
Perhaps the most pervasive myth that is used to push pro-vaxx talking points, that most people believe as a matter of fact is that vaccines were the reason for the decline in death rate from diseases of the 19th and 20th centuries, and namely eradicated smallpox, with marked declines in polio and measles to near eradication. An analysis of the vital statistics of the 19th and 20th centuries from these diseases puts that hypothesis into question. This and this shows that mortality from measles, whooping cough, and various other diseases had already declined by almost 99% BEFORE the vaccine was ever introduced. While with these charts, you usually have the problem of correlation not equalling causation, the fact that the decline happened before the vaccine was introduced means that the vaccine could not have possibly caused it. On the other hand, even if the vaccine had been introduced at around the time that a decline in disease mortality had been seen, you still cannot necessarily conclude that the vaccines caused this decline.
Leicester: Sanitation vs Vaccination: 1912 is an old book that analyzes statistics in an English city called Leicester that chose to not vaccinate their kids against smallpox. It compares their rates of infection and death to other cities with compulsory programs, and the ineffectiveness of these. This book, entitled "The fallacy of vaccination, a doctor of states that smallpox mortality more than doubled after vaccination introduction in England from 7% to 15%
The biggest hysteria behind vaccinating others is on the dogmatic mantra of "herd immunity" and this idea that "my vaccination protects you and your vaccination protects me" (which we see repeated with the COVID mask debacle). However, we see that this does not play out in real life. Hereis a discussion of an outbreak of measles in a fully vaccinated population. China still reports many measles outbreaks despite over 99% population vaccination rate and draconian force vaccination policies. Here we see a mumps outbreak in the highly vaccinated harvard class; note that college students are forced to be up to date on immunizations. The irony of all this, that shows the strength of the dogma, is that when these utter vaccine failures, their assumption is always that we simply need even more vaccines and higher vaccine uptake. That's why their percentage target for herd immunity has steadily increased from 55% to 95% since the 60s for measles. This mumps outbreak occured around a 97% vaccinated group. Here is more of a discussion on the failure of the mumps vaccine.
Here is another good article detailing the failure of the pertussis vaccine, candidly admitted by mainstream sources.Another one from CHD about the influenza vaccine. Here, here, here, and here are just a handful of examples of measles outbreaks thats occur in highly vaccinated populations. In this video at 1:17:10, there are charts presented showing measles outbreaks occuring in populations with vaccination rates as high as 99%.
The most recent vaccine we have, covid, has lots of data on its ineffectiveness and waning effectiveness, mostly from around the world. Qatar shows that after 20 weeks the protection of infection from the vaccine declines to basically 0. This data from the UK shows that the vaccine actually has a negative 73% effectiveness in week 40 through week 43 data of 2021. It is also worth noting that the absolute effectiveness of the vaccine even by the official trials reported by the vaccine manufacturers, are extremely low.
A German friend of mine was able to translate this data from the RKI on breakthrough infections for me. This is roughly his findings. They found a 45% probable vaccine breakthrough rate of COVID deaths among 60+ year olds. The RKI's statement on this is. "Looking at the share of vaccination breakthroughs in all COVID-19 cases, it becomes clear that only a small proportion of hospitalised COVID-19 cases who were cared for in intensive care units or died can be assessed as vaccination breakthroughs. Among the total of 1,076 COVID-19 cases with vaccine breakthroughs from Week 5 to Week 42 who died, 782 (73%) were 80 years and older. This reflects the generally higher risk of death - regardless of the effectiveness of the vaccines - for this age group." They basically write off the high mortality rate as expected because of the high mortality rate of that group in general. The problem with this is that the whole rationale for vaccinating was to protect the vulnerable populations in the first place, and why we had a global lockdown. Now they are writing off deaths from older people as expected. You also see this in the way that people write off potentials for vaccine adverse events among old people. They would say things like "they're old, they're going to die anyway." Where was this attitude for the entirety of the pandemic when we shut down the world to save grandma?
Let's look at a few more examples of vaccine ineffectiveness around this world. In Belgium, this doctor states that 100% of the patients in his ICU are vaccinated. In Sweden, this study shows that the vaccine drow below zero effectiveness by about 200 days. In Illinois, 42% of COVID deaths last week were in fully vaccinated people. In Vermont, 76% of September COVID deaths were vaccinated. In this Irish city with a 99.7% vaccination rate, the highest in Ireland, it has the highest rate of COVID infections in the entire country.
Israel, with one of the highest vaccination rates in the world and some of the strictest vaccination policies, has the highest infection rate in the world. Dr. Kobi Haviv in Israel claims that 85%-90% of hospitalizations are in fully vaccinated people. In Iceland, with 82% of the population fully vaccinated, 77% of new COVID cases are fully vaccinated. In the UK, 70% of COVID deaths are from fully and partially vaccinated people over the age of 50. This CDC study shows that 74% of people infected in a Massachusetts COVID outbreak were fully vaccinated. In Wales, Table 4, 85% of hospitalized COVID patients are vaccinated.
Epidemic of whooping cough in sweden where 84% of the children infected were vaccinated. Measles outbreak in a fully immunized secondary school population. Figure 2, H influenzae meningitis in infants less than 1 year old had already decreased substantially before the introduction of the vaccine in that age group. This shows pertussis infection in fully vaccinated children in Israel. Here is a discussion of a multitude of vaccine failure cases. An article on whooping cough vaccine failures. No recorded cases of measles from 1970 - 1987 among Amish
Moderna and Pfizer recently released their phase 3 trial results. Moderna showed that there was no difference in deaths between the placebo and the vaccine groups, in Table S26. Pfizer showed the same result in Table S4, and also showed twice as many adverse events in the vaccine group in Table S3.
Polio vaccine trial did not use saline placebo, but placebo with phenol red, antibiotics, and formaldehyde
"we published a study demonstrating that among the most highly developed nations, those requiring the most vaccine doses for their infants tended to have the least favorable infant mortality rates"
In this VAERS analysis we looked at 250 of the earliest in which the patient had died, 72% were found to have been authored by a doctor or healthcare employee and included details pasted directly from the EMR
In this follow-up report a year later we reviewed another 1012 VAERS reports in which the vaccine recipient had died, finding in this 4x larger sample 62% were written by healthcare provider staff & most included some information from the patients' EMR
"Thus vaccination does not account for the impressive declines in mortality seen in the first half of the century." "Again, nearly 90% of the decline in infectious disease mortality among US children occurred before 1940, when few antibiotics or vaccines were available."
{kind=link}